All About Collaborative Agreements
I apologize for not putting anything here until now. I am amazed by how many visits this site gets and I am happy to be helping so many people find their way...Thank you for reading!
Now...onto Collaborative Agreements:
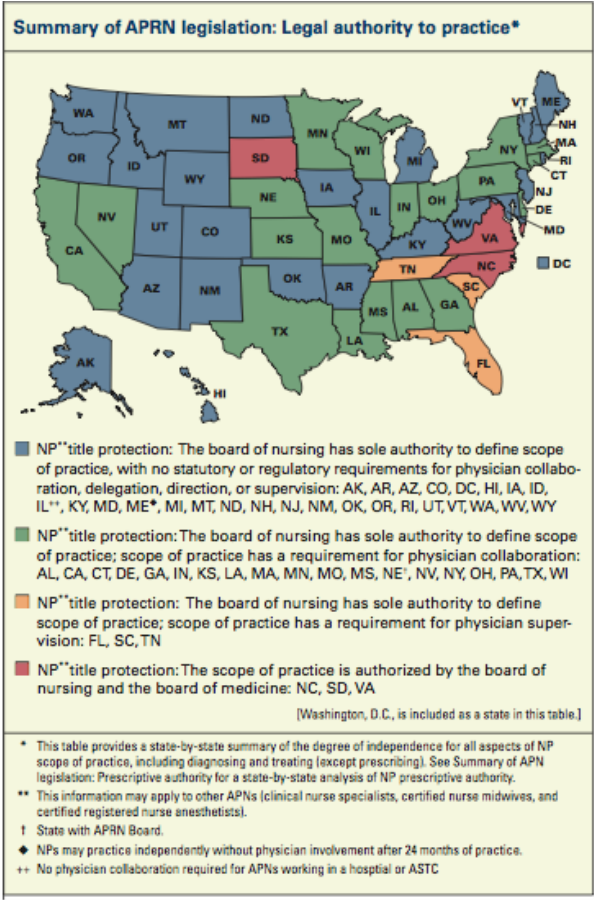
Please check your own state's licensing requirements, as NP practice requirements vary widely from state to state. For the "bible" of NP practice from state to state, I suggest you check out the Pearson Report. This is a state-by-state summary of NP requirements to practice, as well as information on changes in practice from year to year. It is updated and published yearly by a very dedicated and knowledgeable NP and can be found here http://www.pearsonreport.com/overview Linda J. Pearson, DNSc, FPMHNP-BC, FAANP is a Family Psychiatric Mental Health NP who has been publishing the Pearson Report for 22 years. The most current edition of the Pearson Report is not free, however, you can typically find one from a year or two ago online for no charge. I did find an article written in January of 2012 that gives a nice summary of current practice. Here is a link:
http://www.wocn.org/resource/resmgr/Files/APRN_consensus_model_impleme.pdf
Below I posted a picture/summary of state-by-state legislation.
In my home state of Connecticut, APRNs are required to have either an MD or DO as a collaborate physician. Below is information taken directly from the state website:
Scope of Practice
Advanced practice registered nursing is defined as the performance of advanced level nursing practice activities that, by virtue of postbasic specialized education and experience, are appropriate to and may be performed by an APRN. The APRN performs acts of diagnosis, and treatment of alterations in health status and must collaborate with a Connecticut-licensed physician. In all settings, the APRN may, in collaboration with a licensed physician, prescribe, dispense, and administer medical therapeutics and corrective measures and may request, sign for, receive, and dispense drug samples. A licensed APRN maintaining current certification from the American Association of Nurse Anesthetists who is prescribing and administering medical therapeutics during surgery may only do so if the physician who is medically directing the prescriptive activity is physically present in the setting where the surgery is taking place (CGS § 20-87a(b)).
Collaboration
The law defines “collaboration” as a mutually agreed upon relationship between an APRN and a physician who is educated, trained, or has relevant experience that is related to the work of the APRN. The collaboration must address a reasonable and appropriate level of consultation and referral, patient coverage in the absence of the APRN, a method to review patient outcomes, and a method of disclosing the relationship to the patient (CGS § 20-87a(b)).
Concerning an APRN's prescriptive authority, the collaboration between the APRN and a physician must be in writing and must address the level of Schedule II and III controlled substances that the APRN may prescribe. The collaboration must also provide a method to review patient outcomes, including the review of medical therapeutics, corrective measures, laboratory tests, and other diagnostic procedures that the APRN may prescribe, dispense, and administer (CGS § 20-87a(b)).
Notice the areas highlighted in blue. Does this seem a little vague to you? No one sees the collaborative agreement , other than the NP and the collaborating physician. The state does not require a copy, nor do the malpractice insurers or the insurance companies that are billed for patient services. There is no requirement for the physician to ever see a patient, or even see the NP! I've heard of NPs who have never even met their collaborating physicians. They wouldn't even recognize one another if they passed each other on the street!
I'm sure by now some of you are thinking, "So what? Sounds like a good thing. The less involvement the better. why are you even bringing this up?" My problem is this - I am a very honest person (no, really!). What bothers me is that the whole "collaborative agreement" is total B.S. in terms of the patient. It offers a false sense of security to the public. The average person hears about collaborative agreements and falsely assumes that their care is somehow being overseen by a physician. They have no idea what the state requires, and believes that the physician is much more involved in their care than they actually are. This is clearly evident by the blog postings and comments that are written online, both by patients and physicians (or physician wanna-be's).
It is a deceitful and archaic practice that puts an unnecessary burdon on NPs and money in the pockets of physicians (who have done practically NOTHING to earn it). Did I mention that quite often NPs have to PAY physicians to be their collaborators? The going rate is anywhere from $50 per patient to several thousand dollars per month. And the only thing the physician needs to do is sign the agreement and read through a few charts a year. The line that reads "patient coverage in the absence of the APRN..." is misleading. It doesn't mean that the collaborative physician has to cover the NPs patients, just that there has to be another provider available to cover patients (it could be another NP) and it has to be mentioned in the agreement.
The medical community's objection to allowing NP's to practice independently always centers around "patient safety" or some similar B.S. Exactly how does the collaborative agreement protect patients? As a patient, do you feel safer knowing that some MD or DO who lives on the other side of the state- and never even met the NP- breezes through a couple of patient charts a year?
It's time for Connecticut to join the other 26 states who allow NPs to practice independently. Especially since so many of our surrounding states have already done away with the collaborative agreement. (Rhode Island, New Jersey, Vermont, New Hampshire and Maine (after 2 years) all allow NPs to practice independently). New York currently has a bill in its legislature to abolosh the collaborative agreement. Here is a link http://open.nysenate.gov/legislation/bill/S324-2011 As for Massachusetts, the other state that borders Connecticut, I am not sure.
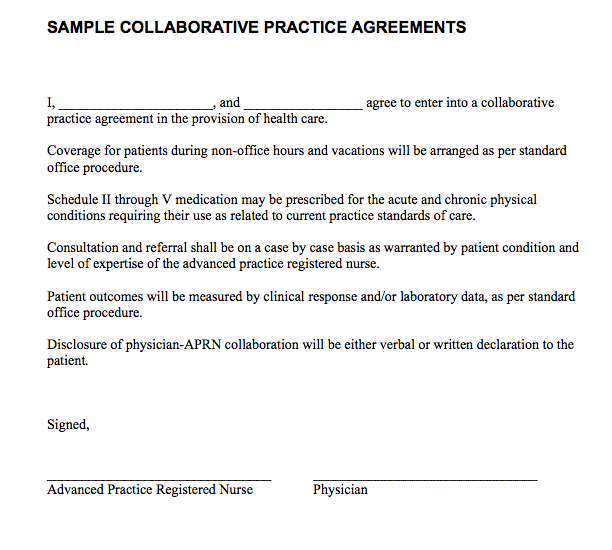
Oh...and just for sh*ts and giggles (what an odd expression!). I posted a copy of a sample collaborative agreement that is actually provided by the State of Connecticut for NPs and physicians to use as a guide. This one really takes the cake! Talk about vague - this gives a whole new meaning to the term! It's taken from a report published in December 2009 by the Connecticut General Assembly 's "Legislative Program Review & Investigations Committee" entitled "Staff Findings and Recommendations - Scope of Practice Determination for Health Care Professions" The full report can be found here: http://www.cga.ct.gov/2009/pridata/Studies/PDF/Scope_of_Practice_F&R.PDF
Thoughts?
Now...onto Collaborative Agreements:
Please check your own state's licensing requirements, as NP practice requirements vary widely from state to state. For the "bible" of NP practice from state to state, I suggest you check out the Pearson Report. This is a state-by-state summary of NP requirements to practice, as well as information on changes in practice from year to year. It is updated and published yearly by a very dedicated and knowledgeable NP and can be found here http://www.pearsonreport.com/overview Linda J. Pearson, DNSc, FPMHNP-BC, FAANP is a Family Psychiatric Mental Health NP who has been publishing the Pearson Report for 22 years. The most current edition of the Pearson Report is not free, however, you can typically find one from a year or two ago online for no charge. I did find an article written in January of 2012 that gives a nice summary of current practice. Here is a link:
http://www.wocn.org/resource/resmgr/Files/APRN_consensus_model_impleme.pdf
Below I posted a picture/summary of state-by-state legislation.
In my home state of Connecticut, APRNs are required to have either an MD or DO as a collaborate physician. Below is information taken directly from the state website:
Scope of Practice
Advanced practice registered nursing is defined as the performance of advanced level nursing practice activities that, by virtue of postbasic specialized education and experience, are appropriate to and may be performed by an APRN. The APRN performs acts of diagnosis, and treatment of alterations in health status and must collaborate with a Connecticut-licensed physician. In all settings, the APRN may, in collaboration with a licensed physician, prescribe, dispense, and administer medical therapeutics and corrective measures and may request, sign for, receive, and dispense drug samples. A licensed APRN maintaining current certification from the American Association of Nurse Anesthetists who is prescribing and administering medical therapeutics during surgery may only do so if the physician who is medically directing the prescriptive activity is physically present in the setting where the surgery is taking place (CGS § 20-87a(b)).
Collaboration
The law defines “collaboration” as a mutually agreed upon relationship between an APRN and a physician who is educated, trained, or has relevant experience that is related to the work of the APRN. The collaboration must address a reasonable and appropriate level of consultation and referral, patient coverage in the absence of the APRN, a method to review patient outcomes, and a method of disclosing the relationship to the patient (CGS § 20-87a(b)).
Concerning an APRN's prescriptive authority, the collaboration between the APRN and a physician must be in writing and must address the level of Schedule II and III controlled substances that the APRN may prescribe. The collaboration must also provide a method to review patient outcomes, including the review of medical therapeutics, corrective measures, laboratory tests, and other diagnostic procedures that the APRN may prescribe, dispense, and administer (CGS § 20-87a(b)).
Notice the areas highlighted in blue. Does this seem a little vague to you? No one sees the collaborative agreement , other than the NP and the collaborating physician. The state does not require a copy, nor do the malpractice insurers or the insurance companies that are billed for patient services. There is no requirement for the physician to ever see a patient, or even see the NP! I've heard of NPs who have never even met their collaborating physicians. They wouldn't even recognize one another if they passed each other on the street!
I'm sure by now some of you are thinking, "So what? Sounds like a good thing. The less involvement the better. why are you even bringing this up?" My problem is this - I am a very honest person (no, really!). What bothers me is that the whole "collaborative agreement" is total B.S. in terms of the patient. It offers a false sense of security to the public. The average person hears about collaborative agreements and falsely assumes that their care is somehow being overseen by a physician. They have no idea what the state requires, and believes that the physician is much more involved in their care than they actually are. This is clearly evident by the blog postings and comments that are written online, both by patients and physicians (or physician wanna-be's).
It is a deceitful and archaic practice that puts an unnecessary burdon on NPs and money in the pockets of physicians (who have done practically NOTHING to earn it). Did I mention that quite often NPs have to PAY physicians to be their collaborators? The going rate is anywhere from $50 per patient to several thousand dollars per month. And the only thing the physician needs to do is sign the agreement and read through a few charts a year. The line that reads "patient coverage in the absence of the APRN..." is misleading. It doesn't mean that the collaborative physician has to cover the NPs patients, just that there has to be another provider available to cover patients (it could be another NP) and it has to be mentioned in the agreement.
The medical community's objection to allowing NP's to practice independently always centers around "patient safety" or some similar B.S. Exactly how does the collaborative agreement protect patients? As a patient, do you feel safer knowing that some MD or DO who lives on the other side of the state- and never even met the NP- breezes through a couple of patient charts a year?
It's time for Connecticut to join the other 26 states who allow NPs to practice independently. Especially since so many of our surrounding states have already done away with the collaborative agreement. (Rhode Island, New Jersey, Vermont, New Hampshire and Maine (after 2 years) all allow NPs to practice independently). New York currently has a bill in its legislature to abolosh the collaborative agreement. Here is a link http://open.nysenate.gov/legislation/bill/S324-2011 As for Massachusetts, the other state that borders Connecticut, I am not sure.
Oh...and just for sh*ts and giggles (what an odd expression!). I posted a copy of a sample collaborative agreement that is actually provided by the State of Connecticut for NPs and physicians to use as a guide. This one really takes the cake! Talk about vague - this gives a whole new meaning to the term! It's taken from a report published in December 2009 by the Connecticut General Assembly 's "Legislative Program Review & Investigations Committee" entitled "Staff Findings and Recommendations - Scope of Practice Determination for Health Care Professions" The full report can be found here: http://www.cga.ct.gov/2009/pridata/Studies/PDF/Scope_of_Practice_F&R.PDF
Thoughts?